Patients Want Convenience. Healthcare Needs to Catch Up.
| Greetmate
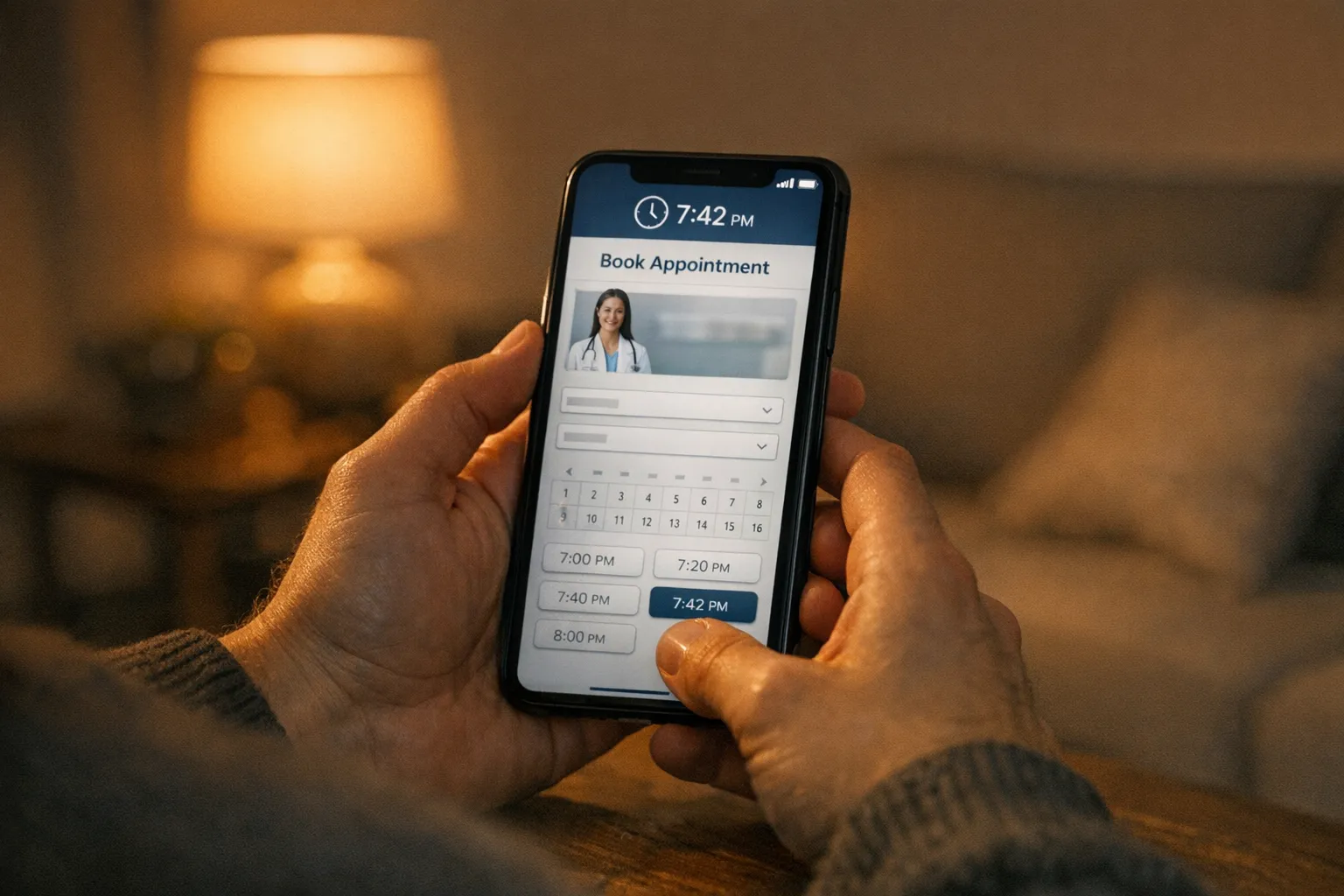
A prospective patient calls a five-location orthopedic group at 7:42 PM after seeing a referral text. The line rings. Voicemail. They hang up, search Google, and book with a competitor by 7:45. That competitor didn't necessarily have better clinicians, a nicer office, or stronger reviews. They had one operational advantage: someone — or something — answered the phone and put an appointment on the calendar.
That is what patient convenience in healthcare actually means in 2026. Not lobby design, not portal aesthetics, not branded apps. It means the practice was reachable, responsive, and able to convert intent into an appointment at the moment the patient was ready to act. And by that definition, most U.S. provider organizations are still behind. Patient expectations have already moved — shaped by banking, retail, and on-demand services — while the operational stack inside practices hasn't kept up.
This article breaks down where the convenience gap really lives, why it costs more than satisfaction scores, and the four operational workflows healthcare leaders need to fix first.
Table of Contents
The Convenience Gap: What Patients Actually Expect Now
Patients now apply the same convenience standard to healthcare that they apply to every other category of service. They expect to book when they want, get answered when they call, and receive a reminder before they have to remember.
What patients now consider baseline:
Booking, rescheduling, or canceling appointments online — at any hour
A phone call answered quickly, not parked in a multi-level IVR
Same-week or same-day availability when clinically appropriate
Digital reminders and confirmations via SMS or email
A response after hours, not a voicemail box
Self-service options for common requests (forms, refills, directions, insurance)
By the numbers: 60% of patients abandon healthcare calls after just one minute on hold. 85% never call back. Most simply book with the next practice that answers.
Why Practices Can't Catch Up (Even When They Try)
Most healthcare leaders know convenience matters. The gap isn't intent — it's infrastructure. Four structural realities make "catching up" harder than it looks:
1. Front-Desk Capacity Is Finite
The same staff that runs check-in, verifies insurance, handles arriving patients, and manages walk-ins also has to answer every inbound call. When call volume spikes — Monday mornings, post-holiday weeks, post-marketing campaigns — the desk can't expand. It just drops calls. We've covered this dynamic in depth in Front Desk Overload: The Real Constraint on Practice Growth.
What "Catching Up" Actually Looks Like Operationally
Closing the convenience gap isn't a marketing exercise. It's an operational one. It requires answering, capturing, scheduling, and following up — reliably, every time, across every location, on every channel.
That means treating patient access the way other industries treat customer infrastructure: as a layer that's always on, integrated with the systems of record, and visible to leadership.
The practical shift looks like this:
24/7 voice + SMS coverage that handles routine intake, scheduling questions, and after-hours overflow without sending callers to voicemail.
Self-scheduling that's integrated with the EHR, not adjacent to it — so what a patient books lands in the calendar staff actually uses.
Digital reminders and confirmations that reduce no-shows without adding desk work.
Multi-location standardization so every site answers and books to the same playbook.
Reporting visibility so leadership can see call answer rates, after-hours volume, booking yield, and conversion by location.
This is the operational layer Greetmate is built for — healthcare voice and SMS AI infrastructure that's implemented, not just activated, and supported, not just self-serve. The goal isn't a "receptionist replacement." It's making sure the practice is reachable and responsive at the moments patients are deciding whether to stay or switch.
Inbound call handling, after-hours coverage, and overflow management.
Appointment scheduling, patient follow-up, and reactivation workflows.
Workflow-driven call logic with EHR and system integrations.
Built for multi-location healthcare groups and partner networks.
The 4 Convenience Workflows to Fix First
You don't have to rebuild patient access in one quarter. You do have to fix the four workflows that drive most of the leakage. In order of operational impact:
1. Inbound Call Answer and Route
The first job is making sure every call is answered — including the second and third calls that arrive while staff are on the first. An AI voice layer can pick up overflow, handle routine requests (scheduling, hours, directions, refill routing), and pass clinically sensitive or complex calls to the right team with full context. This single workflow shift can take a practice from a high single-digit abandonment rate to near zero on routine traffic. For a fuller playbook, see AI Phone Automation for Medical Practices: The 2026 Operations Playbook.
2. After-Hours Coverage
Voicemail is not a strategy. The patient calling at 7:42 PM is not waiting until tomorrow — they're calling the next practice on the list. A 24/7 voice agent that can collect intake, schedule simple appointment types, and triage urgent issues into a documented callback workflow closes the single largest convenience gap in most practices. It also captures the significant share of bookings happening outside business hours that voicemail loses entirely.
3. Confirmations, Reminders, and Reactivation
No-shows are a convenience failure, not a patient failure. Roughly 88% of patients want digital reminders and communication from their providers, and practices that automate confirmations, SMS reminders, and lapsed-patient reactivation see meaningful gains in show rate and slot utilization. This is also where SMS becomes operational, not just promotional — two-way confirmation conversations beat one-way reminder blasts.
4. Intake and Triage Capture
Even when calls are answered, intake quality determines whether they convert. A standardized intake script — captured by an AI agent or routed through a structured workflow — collects insurance, reason for visit, urgency, and preferred time consistently across every site and every shift. That standardization is what makes downstream scheduling, verification, and follow-up actually work. More on this in How to Capture Every Patient Inquiry Without Adding Staff.
Key Takeaways:
89% of patients want to schedule appointments anytime online or by phone — convenience is now a baseline expectation, not a differentiator.
41% of patients would stop seeing a provider over a poor digital experience; 85% never call back after an unanswered first attempt.
67% of patients still prefer calling their provider — fixing the phone channel is as important as building digital options.
40–41% of bookings and calls happen outside business hours; voicemail is not a sufficient operational answer.
The four workflows to fix first: inbound call answer/route, after-hours coverage, reminders/reactivation, and intake/triage capture.
Done right, these four workflows are what patients perceive as "convenient." Done poorly, they're the reason patients leave.
FAQ
What do patients expect from healthcare convenience in 2026?
Patients expect 24/7 self-scheduling online or by phone, calls answered within a minute, digital reminders and confirmations via SMS, easy rescheduling, and a responsive option after hours instead of voicemail. Nearly nine in 10 patients factor convenience features like self-scheduling and texting into their choice of practice.
Will patients really switch providers over inconvenience?
Yes. Research from Cedar found that 41% of patients would stop seeing a provider over a poor digital experience, and one in five already have. Separate research shows around 60% of callers abandon healthcare calls after one minute on hold, and 85% never call back after an unanswered first attempt — most simply book elsewhere.
What's the most cost-effective way to fix after-hours patient access?
For most practices, layering a 24/7 AI voice and SMS agent on top of existing phone lines is more cost-effective and more scalable than expanding call-center headcount. It handles routine scheduling and intake around the clock, escalates urgent issues, and integrates with the EHR so bookings land directly in the calendar staff already uses.
How does this work for multi-location groups?
A centralized AI voice and SMS layer standardizes how every location answers, schedules, and follows up — while still routing to the right local team. Leadership gets visibility into call volume, answer rates, after-hours activity, and booking yield by site, which is usually the missing piece for ops leaders trying to manage access across a group.
Conclusion: Convenience Is an Infrastructure Decision
Patient convenience is no longer a brand attribute. It's the operational difference between the practice that captures a new patient at 7:42 PM and the one that finds out — months later, in a churn report — that the patient went somewhere else.
The practices catching up are not the ones running better satisfaction surveys. They're the ones rebuilding the layer underneath patient access: 24/7 voice and SMS coverage, EHR-integrated scheduling, automated reminders and reactivation, and reporting that lets leadership see what's actually happening across every location. Greetmate exists to make that layer real — healthcare voice and SMS infrastructure that's implemented with white-glove rollout, integrated with the EHRs and tools you already run, and supported as an ongoing operational partnership, not a self-serve trial.
If access is one of your 2026 priorities, the patients are already there. The question is whether your operations are.
See what 24/7 voice and SMS infrastructure looks like for your practice — book a Greetmate demo and walk through a workflow built for your specialty and call volume.
More Blog Articles
Find helpful articles in our blog that are all about business, customer service and AI technology.
Healthcare front desk staff are handling more responsibilities than ever. The right technology should support them, not replace them. Here's what real backup looks like — and how to add capacity without adding headcount.
Interventional pain management practices face crushing prior auth volume, complex procedural coding, and relentless inbound calls. Here are the 6 AI tools actually moving the needle in 2026 — ranked for ops leaders.