The First Practice To Respond Usually Wins
Patients choose the first provider that responds. See the data behind speed-to-lead in healthcare and how to win the access race in 2026.

| Greetmate
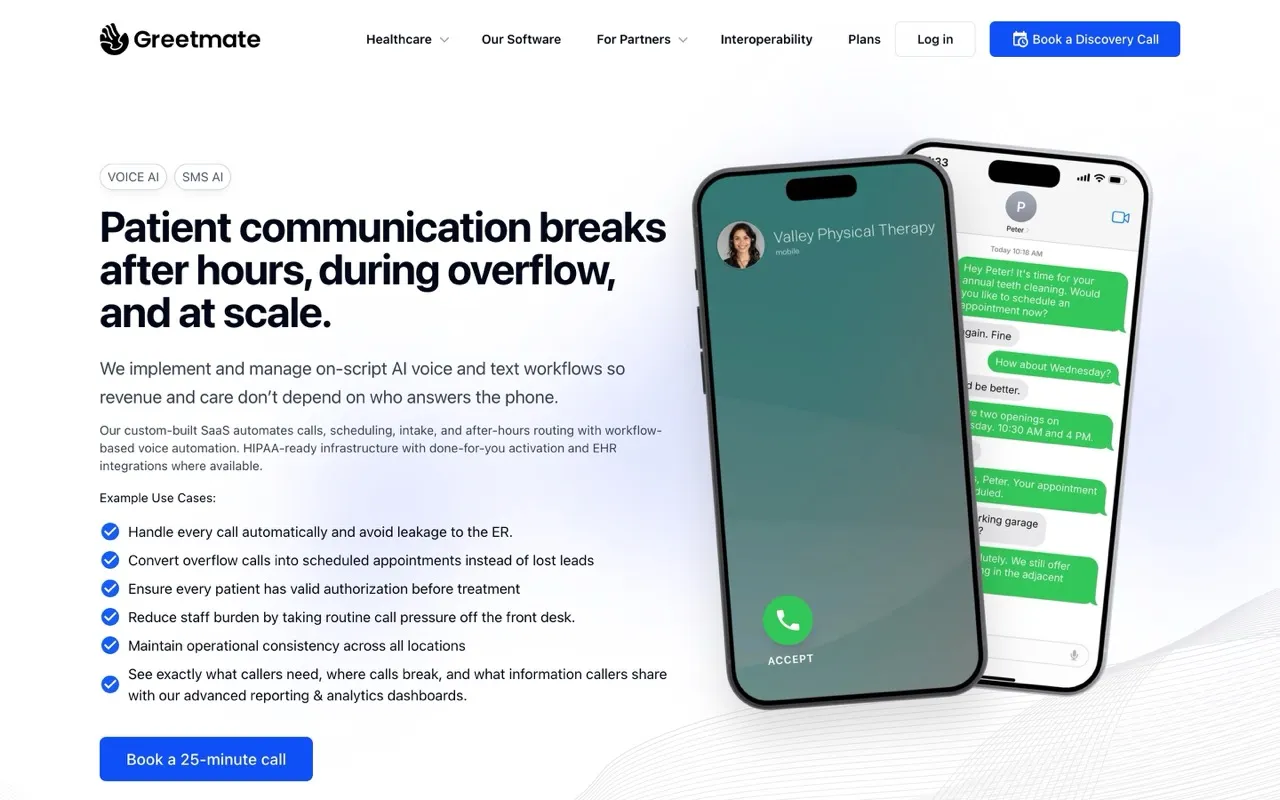
Table of Contents
Key Takeaways:
The phone is still how most patients access care. 88% of healthcare appointments are still booked by phone, with average call durations exceeding eight minutes — and yet the average medical practice misses 23–42% of all inbound calls. That gap between call volume and call capacity is where medical voice AI agents have found their footing in 2026.
This is no longer a category defined by demos and whitepapers. Voice AI is being deployed in production across primary care groups, dental service organizations, behavioral health networks, and multi-location specialty practices. The market is growing at a 37.79% CAGR — one of the fastest in all of health tech. But growth metrics don't tell you whether a given deployment will actually work.
This post covers where medical voice AI genuinely delivers in 2026, what separates infrastructure-grade platforms from demo-ware, where the technology still has real limitations, and what the next 12 months look like for healthcare operations teams evaluating this category.
The global AI voice agents in healthcare market was valued at $468 million in 2024 and is projected to reach $3.18 billion by 2030 — a near 7x expansion in six years. North America currently accounts for 54.17% of global revenue, driven by the combination of chronic staffing shortages, rising patient call volumes, and the maturation of underlying AI infrastructure.
AI Voice Agents in Healthcare: Market Size (USD millions)
But the more meaningful signal isn't market size — it's where the technology sits in the adoption curve. Deloitte's 2026 State of AI survey found that 25% of enterprise leaders now report AI having a transformative effect on their organizations, more than double the prior year. That same survey found that 37% of organizations are still using AI at a surface level, with little change to underlying processes.
For healthcare operations leaders, that gap is the story. The practices and groups seeing real returns from voice AI in 2026 aren't the ones who bought a tool — they're the ones who rebuilt a workflow around it. The distinction matters enormously when evaluating vendors.
Three structural forces are driving adoption specifically in 2026:

What is a medical voice AI agent? A medical voice AI agent is an AI-powered system that handles inbound and outbound patient phone calls autonomously — scheduling appointments, capturing intake information, routing calls, sending SMS follow-ups, and writing data back to the EHR — without requiring a human staff member to be on the line.
That definition covers the concept. What it doesn't capture is the operational distance between a voice AI agent that answers calls and one that actually resolves them.
In 2026, production-grade medical voice AI handles six core workflow categories:
This is a critical distinction that vendor marketing often blurs. A traditional IVR (interactive voice response) system routes calls using pre-written scripts and keypad inputs. It doesn't resolve anything — it transfers it.
An AI voice agent conducts a real conversation. It understands patient intent from natural speech, handles mid-call topic shifts, applies scheduling logic, and writes outcomes back to connected systems. At certain U.S. hospitals, AI-powered assistants now manage more than 60% of inbound scheduling calls — not by routing them to humans faster, but by handling them end-to-end.
The practical difference: a patient calling to reschedule with an IVR gets transferred to hold. A patient calling to reschedule with a capable AI agent gets rescheduled in under two minutes, receives an SMS confirmation, and never speaks to a human — unless they want to.
Scheduling is the highest-volume use case, and the ROI case is straightforward. Some large medical groups have successfully automated over 50% of their front-desk call volume for scheduling using AI, dramatically reducing call backlogs and eliminating hold queues.
On the no-show side, medical practices using AI intake saw a 40% reduction in no-show rates — driven by automated, conversational SMS reminders that allow patients to confirm or reschedule without playing phone tag with a coordinator.
Inbound Call Outcomes: AI-Enabled Medical Groups
This is arguably where voice AI delivers the most immediate, measurable value for group practices and multi-location organizations. The math is direct: every call that hits voicemail after 5 PM is a potential lost patient. 85% of patients who reach voicemail will not call back. Multiply that across 20 after-hours calls per night across 5 locations, and you're looking at a compounding revenue leak.
AI voice agents eliminate that leak by answering every call — at 7 PM, 2 AM, or during a Monday morning surge — capturing appointment requests, routing urgent calls appropriately, and sending SMS confirmations. The agent doesn't call in sick. It doesn't take a lunch break.
Automated voice calls cost 10–15% of what a live agent call costs, and platforms routinely achieve 50%+ call deflection rates in production — meaning more than half of all calls are fully resolved without human involvement.
Outbound workflows are underutilized in most practices — not because the value isn't there, but because coordinators don't have time to work a recall list manually. Voice AI changes the economics of outbound entirely.
Automated recall campaigns, post-visit follow-up calls, and reactivation sequences for patients who haven't been seen in 12+ months can run continuously in the background, without coordinator time. The calls that need human follow-up get flagged and routed. The rest are handled.
Platforms like Greetmate are built specifically for this — automating 70–80% of routine patient communication tasks so coordinators focus on the calls that actually require human judgment.
Here's the uncomfortable reality: 78% of enterprises have at least one AI agent pilot running, but only 14% have reached production scale — and in healthcare specifically, that production deployment rate drops to just 8% — the lowest of any sector surveyed.
AI Agent Pilot-to-Production Rate by Sector (2026)
The gap between a compelling demo and a reliable production deployment comes down to four factors.
Most vendors offer "EHR integration." What that means in practice varies enormously. There is a wide gap between a basic API connection that reads availability and a bi-directional integration that reads patient records, checks live scheduling logic across provider types and locations, writes appointment data back in real time, and handles cancellation and rescheduling workflows without creating duplicate records.
96% of hospitals have adopted FHIR APIs, which creates the technical foundation for deep integration — but most voice AI vendors are still operating at the surface layer. Ask any vendor you evaluate: does the integration write back to the EHR, or does it only read from it? What happens when a scheduling conflict occurs mid-call?
Greetmate's interoperability layer connects to 300+ applications — including athenahealth, Epic, ModMed, Tebra, eClinicalWorks, Dentrix, Open Dental, Canvas, and DrChrono — with bi-directional data flow built for operational workflows, not just demos.
HIPAA compliance in voice AI is not binary. A vendor can technically sign a Business Associate Agreement (BAA) while still having significant gaps in how PHI is handled during call transcription, storage, and third-party model routing.
What to evaluate: end-to-end encryption, role-based access controls, full audit logging, PHI redaction in transcripts, and how data flows through any third-party AI model providers used by the platform. A BAA is the starting point — not the finish line.
Greetmate is HIPAA-ready with BAA available, built from the ground up for healthcare communication workflows — not retrofitted from a general-purpose voice platform.
A voice AI agent that answers a call and schedules an appointment is doing the minimum. What happens next is where most platforms fall short.
Does the platform trigger an SMS confirmation? Log the call outcome? Flag missed-call opportunities for follow-up? Route the call summary to the right coordinator? Update the patient record? Generate scheduling outcome reports across locations?
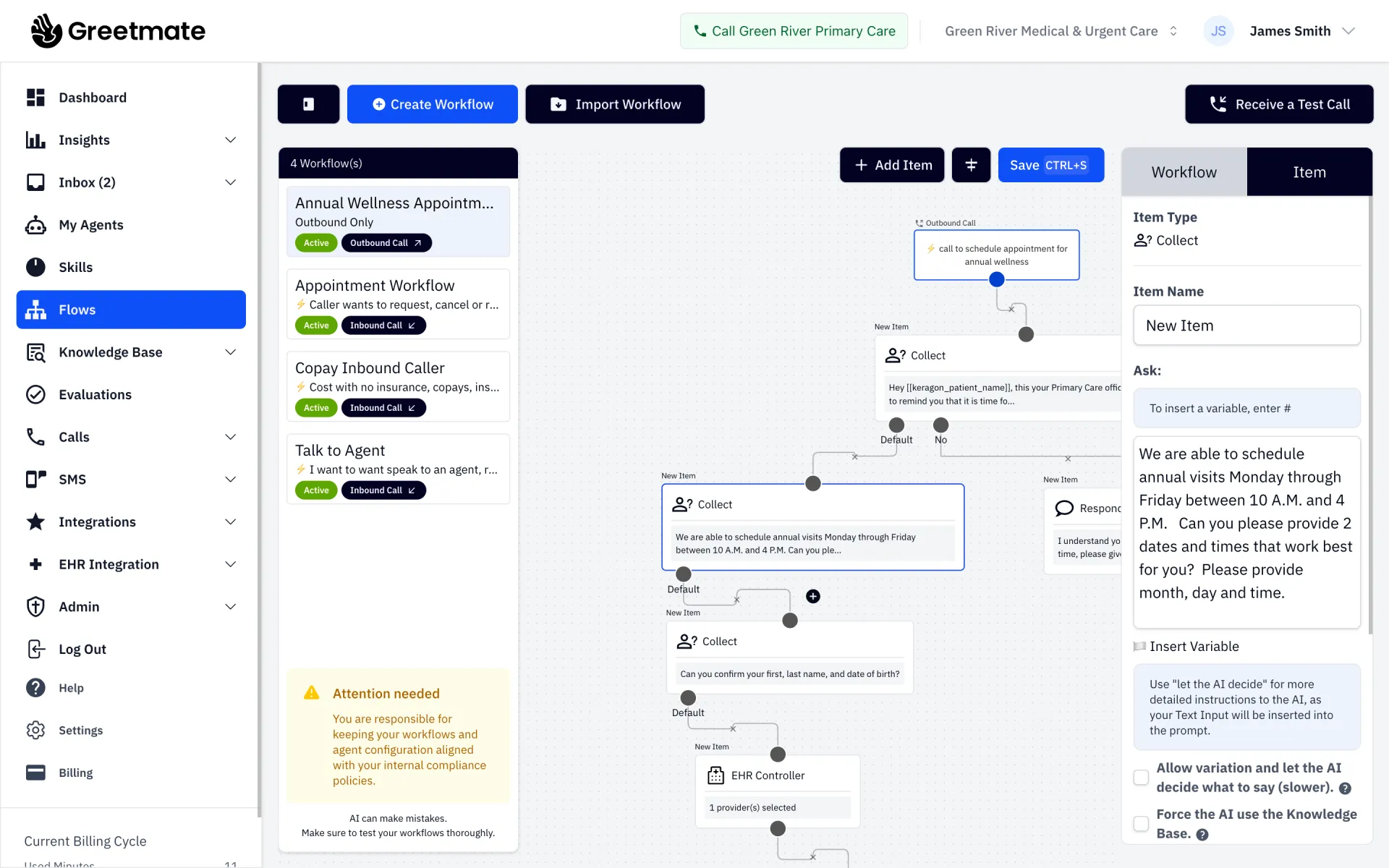
This is the difference between a call-answering tool and communication infrastructure. The Greetmate software platform is built around this depth — no-code workflow builder, custom call flows, intake capture, triage routing, reporting, and SMS coordination all connected in a single operational layer.
This is the buying decision factor almost no vendor comparison covers honestly. A self-serve platform puts workflow configuration, EHR integration setup, call flow design, and testing on your team. For a 2-location practice with a tech-savvy office manager, that may be fine. For a 15-location DSO or an MSO managing workflows across 30 practices, it isn't.
Managed implementation — where the vendor builds and configures the workflows, integrates the systems, and handles the operational setup — is what closes the gap between pilot and production. It's also what the 80% failure rate data points to as the primary driver of stalled deployments.
Greetmate offers both: a self-serve software platform for teams that want to build their own workflows, and a white-glove managed implementation where Greetmate builds the entire workflow and automation layer — delivering operational value fast, without putting the configuration burden on your team.
Reduce front-desk call volume and improve patient communication.
Go live in hours with done-for-you setup.
Any honest state-of-market analysis has to address the limitations. Here's where the technology still has real gaps in 2026:
Latency under real-world conditions. The gold standard for conversational voice AI is ultra-short response time. Leading platforms are achieving this in controlled environments. But latency in voice AI is a user experience failure, not just a performance metric — pauses beyond 1.5 seconds feel like dropped calls, and users hang up. Real-world telephony introduces jitter, packet loss, and audio quality variation that can push effective latency well above benchmark numbers. Evaluate vendors on production latency, not lab latency.
Turn detection fragility. The AI needs to know when a patient has finished speaking before it responds — without interrupting and without waiting too long. This sounds simple and is technically hard. Patients who pause mid-sentence, speak with accents, or use complex phrasing still trip up many systems. Specialist models trained on healthcare-specific audio show up to 70% fewer errors compared to general-purpose models — which is why healthcare-native platforms have a real advantage over generic voice AI tools.
Complex multi-intent calls. A patient who calls to reschedule, asks about their insurance, and mentions a prescription refill in the same call is testing the limits of most current systems. Generic platforms handle these as isolated intents and either misroute or escalate. Healthcare-native platforms handle this better, but multi-intent resolution in a single call remains an area of active development.
EHR write-back reliability. Reading from an EHR is relatively straightforward. Writing back — creating appointments, updating records, handling conflicts — introduces complexity that breaks many integrations at scale. This is the single most common cause of failed production deployments.
Clinical nuance and escalation judgment. Voice AI handles operational workflows. It does not — and should not — handle clinical judgment calls. The platforms that work well have clear, well-designed escalation paths that route calls to human staff when clinical context is needed. This isn't a limitation to engineer around; it's a design principle to build in.
Bottom line on limitations: The practices that get the most out of voice AI in 2026 are the ones who deploy it within its reliable range — routine scheduling, intake, after-hours coverage, reminders — and design thoughtful escalation paths for everything outside that range. The technology is a powerful operational lever, not a replacement for clinical judgment.
Several developments will define the voice AI landscape in healthcare through early 2027:
EHR-native AI will expand. Epic is launching 150+ AI features built directly into its platform. athenahealth is making ambient AI available to all users at no additional cost. Oracle Health is rolling out AI agents across revenue cycle, nursing, and clinical operations. This matters for the voice AI category because it raises the integration bar — platforms that only operate at the API surface layer will face increasing competition from EHR-native capabilities.
The managed-vs-self-serve divide will sharpen. As the technology matures, the buyers who got the most value from voice AI in 2025–2026 will be the ones who had full-stack implementation support — not the ones who bought a SaaS license and configured it themselves. Expect more platforms to move toward managed deployment models to close the pilot-to-production gap.
Multi-location and MSO deployments will accelerate. The ROI case for voice AI compounds with scale. A 3-location group saves coordinator time. A 20-location group standardizes call handling, eliminates location-level variation, and gains cross-portfolio reporting. Greetmate's multi-location infrastructure is built specifically for this — consistent workflows, centralized reporting, and EHR integrations that work across locations rather than being configured site by site.
Partner-channel growth. Medical answering services, RCM companies, and healthcare MSPs are increasingly embedding voice AI into their service offerings rather than building it from scratch. The economics are compelling: AI handles the routine volume; human agents handle the escalations. Greetmate's partner program is designed exactly for this model — giving operations partners the infrastructure to deploy AI voice across their client base without building a platform themselves. See also: Partners: Medical Answering Services.
Gartner projects that over 40% of agentic AI projects will be canceled by end of 2027 due to escalating costs, unclear business value, and inadequate risk controls. The practices and groups that avoid that fate will be the ones who deployed against specific, measurable operational problems — not the ones who deployed because it seemed like the right time to have an AI strategy.

What is a medical voice AI agent?
A medical voice AI agent is an AI-powered system that handles inbound and outbound patient phone calls autonomously — scheduling appointments, capturing intake information, routing calls, triggering SMS follow-up, and writing data back to the EHR — without requiring a human staff member to be on the line for routine interactions.
Are medical voice AI agents HIPAA compliant?
Purpose-built healthcare voice AI platforms can be HIPAA compliant, but compliance requires more than a signed BAA. Evaluate end-to-end encryption, role-based access controls, full audit logging, PHI handling in call transcripts, and how patient data flows through any third-party AI model providers. Platforms like Greetmate are HIPAA-ready with BAA available, built from the ground up for healthcare communication workflows.
How much call volume can a voice AI agent handle?
Production deployments routinely achieve 50%+ call deflection rates — meaning more than half of all inbound calls are fully resolved without human involvement. After-hours and overflow coverage is typically the highest-deflection use case, since those calls would otherwise go to voicemail. The agent handles unlimited concurrent calls, eliminating the capacity constraints of a fixed front-desk team.
What EHR systems do medical voice AI agents integrate with?
Integration depth varies significantly by vendor. Leading healthcare-native platforms integrate with major EHRs including athenahealth, Epic, ModMed, Tebra, eClinicalWorks, Dentrix, Open Dental, Canvas, and DrChrono. The key question to ask is whether the integration is bi-directional — reading from and writing back to the EHR in real time — or read-only.
Why do so many voice AI deployments fail to scale?
The March 2026 data is clear: 78% of enterprises have AI agent pilots, but only 14% have reached production scale — and in healthcare, that drops to 8%. The primary failure modes are shallow EHR integration that breaks at scale, inadequate implementation support that leaves workflow configuration to internal teams, and unclear escalation paths when the AI encounters edge cases. Managed implementation — where the vendor builds and owns the workflow layer — is the most reliable path from pilot to production.
Medical voice AI is past the proof-of-concept stage. The market is growing, the technology is maturing, and the operational case — missed calls, after-hours gaps, front-desk overload, multi-location inconsistency — is well-documented. But the gap between a vendor demo and a production deployment that actually reduces front-desk burden and recovers revenue is still wide, and most organizations are finding that out the hard way.
The practices and groups that are winning with voice AI in 2026 are the ones who deployed against specific operational problems, chose platforms with genuine EHR depth, and had real implementation support. That's the standard Greetmate is built to meet — 35%+ front-desk workload reduction, 70–80% routine task automation, and a white-glove managed implementation model that delivers operational value without putting the configuration burden on your team.
Handle patient calls around the clock — including after-hours and overflow — so your front desk can focus on in-office care.
Automate appointment scheduling, patient follow-ups, and reactivation outreach through workflow-driven voice communication.
Connect with your existing EHR, scheduling tools, and operational systems for seamless, end-to-end patient communication.
See Greetmate in Action.
Healthcare voice AI infrastructure — live in hours.
Find helpful articles in our blog that are all about business, customer service and AI technology.
Patients choose the first provider that responds. See the data behind speed-to-lead in healthcare and how to win the access race in 2026.
Every delayed callback costs revenue. See the math behind faster patient response times — and the operational levers that turn access into ROI.
